Uterine fibroid embolisation is a minimally invasive treatment for symptomatic uterine fibroids. It is less invasive and has lower rates of complications and recovery time than either hysterectomy or myomectomy and often provides an excellent alternative to surgery.
Fibroids are nodular overgrowths of muscle and fibrous tissues that occur in the uterus. As many as 25% of women in the reproductive age group will have one or more fibroid. Fibroids are not malignant or cancerous (except in extremely rare cases). The great majority of fibroids do not cause symptoms but are a chance finding on an ultrasound of the uterus being performed for some other reason. These asymptomatic fibroids are usually of no clinical significance.
Fibroid Classification
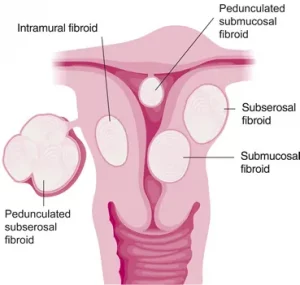
Fibroids are classified according to their position in the wall of the uterus (see figure 1). The most common locations are:
- Submucosal (lying immediately under the endometrium which lines the cavity of the uterus)
- Intramural – lying within the muscle of the uterus and not distorting the endometrium or cavity of the uterus
- Subserosal – lying immediately under the outer lining (or serosa) of the uterus
Less commonly, the fibroid can be “pedunculated” or on the end of a stalk. These can be either:
- Pedunculated submucosal – Hanging inside the uterine cavity on a stalk
- Pedunculated subserosal – hanging off the outer surface of the uterus and dangling in the pelvis
Very commonly there are multiple fibroids scattered throughout the uterus. These are often a mixture of submucosal,intramural and subserosal.
Fibroid Symptoms
Fibroids can cause symptoms due to pressure if they grow to sufficient size. These symptoms can be:
- Heavy bleeding periods (menorrhagia) due to pressure on the endometrium.
- Painful periods due to enlargement and distortion of the shape of the uterus
- Pressure symptoms on the urinary bladder or bowel due to general enlargement of the uterus.
- Protuberant belly due to enlarged uterus.
Treatment for symptomatic fibroids includes:
- Hormone therapy to try to shrink the fibroid
- Uterine fibroid embolisation (UFE)
- Surgical myomectomy
- Surgical hysterectomy
If the symptoms are of sufficient disturbance to lifestyle as to warrant an intervention, then there is a choice between surgery and uterine artery embolisation. If fertility is a major priority then the fertility rate after myomectomy appears better than the fertility rate after UAE.
If future fertility is less important, then UAE provides similar efficacy to myomectomy but is a much less invasive procedure, has lower risk of complication, has a shorter recovery period. It has similar rates of improvement in blood loss and pelvic pain.
UAE is also an excellent alternative to hysterectomy in women who wish to avoid such surgery. 80% of patients can obtain good symptomatic relief from pain, heavy bleeding and pelvic pressure symptoms with UAE. The recovery is much quicker than hysterectomy, the complication rate is lower and the uterus is preserved.
Uterine Artery Embolisation Technique.
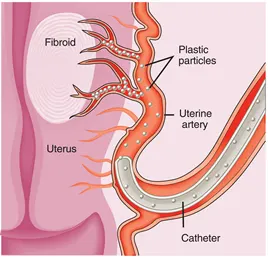
The procedure does not hurt. A light sedative is given to allow the patient to relax. Local anaethetic is administered to the top of the right leg. A thin plastic tube (“angiogram catheter”) is passed into the artery at the top of the right leg. This tube is 1mm in diameter. There is no wound and no scar. The tube is passed into each internal iliac artery using imaging guidance to track the position of the tube. The patient cannot feel the tube inside the arterial system. A finer tube 9measuring 0.8mm diameter) is then passed into the horizontal part of the left uterine artery. Contrast is injected to obtain an angiogram image of the uterus and fibroids (See Figure 2)

Particles are injected into the uterine artery. These particles are 500 microns (1/2mm) in diameter. They flow down the uterine artery and block up the arteries at the 0.5mm level of artery diameter. This type of embolisation will kill the fibroids (which have a precarious blood supply) but will not damage the normal tissues of the uterus. When the left uterine artery is blocked the fine micro-catheter is repositioned in the horizontal segment of the right uterine artery and the particles are injected into the right uterine artery to block the outflow at 0.5mm level of arterial diameter (See Figure 3).
The entire procedure takes about 45 minutes and is painless. The discomfort of the “post-embolisation syndrome” begins about 30 minutes after the embolisation.
Post-embolisation syndrome
The post-embolisation syndrome is caused by damage to the fibroids caused by cutting off their blood supply. As the fibroids die they cause pain. This is usually felt similar to a period pain but more severe. We treat this pain with non-steroidal anti-inflammatory either as tablets or suppositories as well as injections of narcotics such as pethidine, morphine or fentanyl depending on patient preference. The more severe pain normally lasts 12 – 24 hours but is well controlled with medication. It is often advisable to have one night in hospital for pain relief and then be discharged home the day after the procedure. Pain tablets such as digesic or panadeine forte will be supplied to ease further discomfort. The post-embolisation syndrome progressively subsides over one week.
Women are advised to allow one week off work to recover from the procedure.
What are the pre-procedural evaluations required?
- All patients will be required to have a pre-procedure consultation by the interventional radiologist. This allows us to obtain a gynecologic and general medical history, a brief physical examination, and to review the imaging findings and to discuss the procedure with the patient.
- A recent ultrasound of the pelvis is required. Occasionally a CT or MRI scan will also be needed if the ultrasound imaging is not clear.
Do I need to see a gynaecologist?
You need to be jointly cared by an interventional radiologist and a gynaecologist, in conjunction with your GP. You need to see your own gynaecologist or we can recommend one to you for the following assessment:
- A pelvic examination by a gynecologist within six months of the procedure.
- A Pap smear within the last year and should be normal.
- If you have abnormal uterine bleeding (periods lasting longer than 10 days or periods more frequently than every 21 days), an endometrial (inner lining of the uterus) biopsy is needed, preferably within the preceding 3 to 6 months. This is to be certain that the bleeding is not due to abnormal growth.
- If you have a history of pelvic infection, cultures for Gonorrhea and Chlamydia need to be obtained.
Your gynaecologist will also take part in your recovery and follow-up, as well as your on-going well women care.
What are the preparations needed?
On the day of your procedure, you need to avoid solid food from midnight. Clear fluid and medications are allowed up to the time of procedure. We will start an intravenous line to give you fluid, sedatives and pain relief medications. You must not be pregnant. A pregnancy test is needed if the procedure is done more than 10 days since the beginning of your last menstrual cycle. Full blood count and FSH will be obtained before the procedure.
We also need to place a catheter in your bladder, so that the bladder will remain empty during the procedure. Since the bladder is directly in front of the uterus, X-ray dye collected in the bladder would obscure our view.
We will arrange PCA (Patient Controlled Analgesia) pump through an anaethetist.
How do I recover after UFE?
After the procedure, you will be given PCA (patient controlled analgesia) pump that allow youself to administer the dose you need. You will be resting in the ward for one to two days. If you like you can sit in a chair or walk around from two hours after procedure. You might experience varying degree of pain, nausea and fever. Medications are prescribed to control these symptoms. You may eat and drink immediately after the procedure, if you feel up to it.
What are the follow-ups required?
We will call you the day after discharge and again a week after discharge. You should see your gynaecologist 1-2 weeks after the procedure to let him/her know your progress and to manage any gynaecological problems. For minor symptoms and other medical problems, you should visit your regular GP.
What do I need to watch for potential problems?
Redevelopment or resurgence of abdominal pain or fever, or development of foul smelling vaginal discharge might indicate either an infection or sloughing of fibroid. You may require gynecologic evaluation. If any of these symptoms occur, please try to contact us immediately, or present to your GP or gynaecologist. It the symptoms are serious and urgent (eg after hours), you should present to emergency department for initial assessment and ask the emergency doctors to contact interventional radiologist and your gynaecologist for advice.
Links
Further information can be found at the following links:
http://www.sirweb.org/patients/uterine-fibroids
http://www.cirse.org/files/File/UFE.pdf
http://www.rsna.org/Publications/rsnanews/june06/uterine_june06.cfm